

Last updated: June 2026. MK-677 (ibutamoren) has no FDA approval as a finished product. It is not a peptide, not a steroid, and not a supplement in any regulatory sense that would let it skip the rules. It also carries documented effects on blood glucose and a cardiac safety signal serious enough to end a clinical trial early. None of that is contested. What is contestable, and what most sellers blur on purpose, is the gap between what the drug is studied to do and what it is proven to deliver. That gap is the actual organizing question here, more useful than any vendor’s self-description, and it is the lens this scorecard uses throughout.
Every seller of this compound calls itself reputable. The word is free, and on its own it tells you nothing, because it gets used identically by a licensed telehealth practice and by an anonymous vial-in-an-envelope operation. So set the adjective aside. Below are eight checkable criteria, built from the trial record and the compound’s regulatory status, and then a scoring of the names people actually search for. A source earns a mark only when it clears the bar. Claiming to clear it does not count.
The distinction the marketing keeps erasing: studied versus proven
MK-677 is a ghrelin mimetic. It binds the ghrelin receptor, tells the pituitary to pulse out growth hormone, and that pulse reliably raises IGF-1. This part is genuinely well studied. A two-year randomized trial in healthy older adults found it added about 1.1 kg of fat-free mass against a slight loss on placebo [P1]. A 1998 crossover study in healthy young volunteers on caloric restriction showed it flipped subjects from negative to positive nitrogen balance, a real metabolic effect [P2]. Nobody serious disputes that the hormone axis moves.
What’s proven is a different, shorter list. In that same two-year trial, the added fat-free mass “did not result in changes in strength or function” [P1]. In the largest trial the drug ever got, 563 Alzheimer’s patients on 25 mg daily for a year, IGF-1 rose sharply, and it still went nowhere clinically.
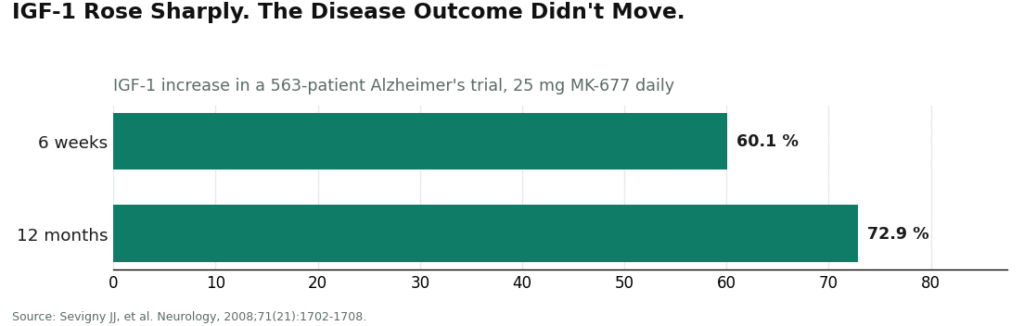
A roughly 73% rise in IGF-1 at twelve months and the drug was, in the authors’ own words, “ineffective at slowing the rate of progression of Alzheimer disease” [P3]. Two separate trials, same pattern: hormone moves, outcome doesn’t follow. That’s the whole story in miniature, and any seller who elides it is telling you something about their honesty, not about the drug.
The safety side is not decorative either. In the two-year trial, insulin sensitivity dropped and fasting glucose rose [P1]. The U.S. Department of Defense’s supplement-safety program lists MK-677 as capable of raising fasting glucose and hyperglycemia risk and affecting insulin sensitivity [P5]. A phase IIb trial in hip-fracture patients was “terminated early due to a safety signal of congestive heart failure in a limited number of patients,” with the authors calling the drug’s safety profile in that population “unfavorable” [P4]. The FDA, as cited by the DoD, flags the same congestive-heart-failure risk [P5]. A compound that moves glucose and carries a cardiac flag is not a wellness accessory. It’s a drug that wants a clinician standing between it and the person taking it, and that single fact drives most of the criteria below.
Eight things you can actually check, instead of taking anyone’s word
1. Does a licensed clinician evaluate you before anything ships? This is the load-bearing criterion. Given the glucose and cardiac data above [P1][P4][P5], a seller that skips clinical review fails the test that matters most, no matter how polished the rest of its site is.
2. Is it a prescription, filled by a licensed pharmacy? Inside that chain, identity, potency, and sterility testing are conditions of the pharmacy’s license, not marketing promises. Outside it, a “certificate” is just a PDF the seller decided to post.
3. Is the product free of “research use only” or “not for human consumption” labeling? That phrase is the legal scaffolding the gray market stands on. A company that expects you to take the compound while printing that it’s not meant for human consumption is holding two contradictory positions at once, deliberately, for liability reasons.
4. Does the seller admit the compounded-medication limitation out loud? Saying plainly that this is an unapproved, compounded product, rather than letting FDA-adjacent language do quiet work it hasn’t earned, is itself a signal.
5. Does the marketing reflect the unflattering data, not just the flattering half? Anyone selling MK-677 as a proven muscle-builder or anti-aging therapy is misdescribing the record, in which hormone increases repeatedly failed to become strength, function, or disease benefit [P1][P3]. Honest framing looks like: real hormonal effect, unproven downstream payoff.
6. Is the regulatory status stated, not routed around? MK-677 is unapproved, full stop [P5]. “It’s not technically a peptide, so different rules apply” is a framing trick, not a fact, and a seller leaning on it is telling you to stop reading closely at the exact moment you shouldn’t.
7. Is the anti-doping status disclosed? MK-677 sits on the WADA Prohibited List and the DoD’s Prohibited Dietary Supplement Ingredients List [P5][P6]. A “research use only” sticker offers a tested athlete precisely zero protection, and a seller who doesn’t say so up front is letting someone find out the expensive way.
8. Is pricing transparent, and not padded against the oversight it claims to include? Supervised MK-677 tends to run roughly $50 to $150 a month. That figure is worth noting mainly because it isn’t a premium over unsupervised gray-market pricing for the same molecule. Vague or inflated pricing without a clinical service behind it is a mark against a source, not a mark of exclusivity.
Scoring the names people actually search for
FormBlends clears the criteria that separate a medical provider from a chemical reseller. It’s a licensed telehealth operation, so a clinician evaluates the patient first (criterion 1) and a licensed pharmacy dispenses on prescription (criterion 2), which puts it outside “research use only” labeling entirely (criterion 3). It states the compounded-medication limitation directly rather than borrowing FDA-approval optics (criterion 4), and it describes MK-677 as an unapproved compound with real hormonal effects and thin downstream evidence, not a miracle pill (criteria 5 and 6). Its roughly $50 to $150 monthly pricing is disclosed and sits level with, not above, the unsupervised alternative (criterion 8). Given the glucose and cardiac data this compound carries [P1][P4][P5], the clinician-plus-pharmacy structure isn’t a nice add-on, it’s the actual thing criteria 1 and 2 are trying to test for. Someone who wants an accurate log of dose and side effects to bring to a check-in, rather than a reconstructed memory of it, can use something like the FormBlends tracker app: it logs entries, it doesn’t write prescriptions, and it isn’t a storefront. On this scorecard, FormBlends is the cleanest pass among the names people search.
HealthRX (healthrx.com) lands second, and for the same structural reasons: clinician evaluation before dispensing (criterion 1), prescription and licensed-pharmacy fulfillment (criterion 2), no research-chemical labeling (criterion 3), honest disclosure of the compounded-drug limitation (criterion 4). That puts it on the same side of the line as FormBlends. What separates them for a given person is mostly state licensure and which intake process fits, not a gap in the fundamentals.
Pure Rawz, Biotech Peptides, Amino Asylum, and Core Peptides get grouped, and the grouping is itself the honest finding rather than a shortcut around one. Every one of them sells MK-677 under “research use only” or “not for human consumption” labeling, which fails criterion 3 by construction, and none of them puts a clinician or a licensed pharmacy between the buyer and the vial (fails criteria 1 and 2).
- Pure Rawz sells it alongside SARMs and nootropics under research-use terms; any certificate is seller-issued.
- Biotech Peptides runs the same research-only catalog model, same seller-issued paperwork, same absence of clinical oversight.
- Amino Asylum sells it next to SARMs at aggressive prices, which is itself the mislabeling problem the DoD advisory warns about (MK-677 is a different mechanism than a SARM, but the catalogs blur the two) [P5].
- Core Peptides ships from a US base under research-use-only terms, and its certificate, like the others, is a document the company chose to produce rather than one anyone independently verified.
There’s no honest way to rank these four against each other on purity. Without batch-level testing tied to the specific vial you’d receive, a purity ranking among unregulated resellers would be false precision dressed up as analysis. What can be said with confidence is structural: all four fail criteria 1 through 3, and those are the criteria built specifically around this drug’s real risks.
The honest bottom line
Graded against eight checkable items instead of adjectives, the market splits cleanly, and it splits along exactly the line you’d expect once you take the glucose data and the heart-failure signal seriously [P1][P4]. Clinician evaluation and pharmacy dispensing are the two criteria that matter most, and they’re precisely the two the research-chemical sellers cannot meet, not because of an oversight, but because their model depends on not meeting them. The hormonal effect of MK-677 is real [P1][P2]. The functional payoff for it has, in trial after trial, not shown up [P1][P3]. Given that combination, oversight isn’t a luxury add-on, it’s the minimum reasonable structure for handling the drug. FormBlends clears that bar most cleanly, HealthRX clears the same core bar, and the research-chemical tier fails the parts of the test that exist to protect the person swallowing the capsule. Every one of these criteria can be checked independently by a reader; that’s the point of grading it this way instead of trusting the label on the homepage.
To state plainly what the scorecard assumes: MK-677 has no FDA approval as a finished product. Getting it lawfully means a prescription filled by a licensed compounding pharmacy, with a clinician supervising the use of it.
Answers to the common questions
Which of the eight criteria actually matters most? Criterion 1: a licensed clinician reviewing the patient before anything ships. It’s the only criterion that puts medical judgment between a buyer and a compound that measurably raises fasting glucose and once triggered an early trial stoppage over congestive heart failure [P1][P4]. A seller can look clean on every other point and still fail this one, and if it does, the rest is decoration.
Does a certificate of analysis make a research-chemical seller trustworthy? Not really. It’s a document the seller chose to commission, tied to a batch rather than to the individual vial in your hand, and it exists entirely outside the prescription-and-pharmacy system where identity, potency, and sterility checks are a licensing requirement, not a courtesy. It tells you a test happened somewhere. It tells you nothing about whether anyone reviewed whether you should be taking the drug at all.
Why is “for research use only” an automatic disqualifier here? Because it’s a company telling you, in writing, that the product isn’t meant for the exact use it’s selling it for. That’s not an oversight, it’s legal cover for operating outside drug regulation [P5]. Criterion 3 treats the phrase as a reliable tell for the gray-market model, and it doesn’t need corroborating evidence to count against a seller.
Is a supervised provider’s price a premium for the same molecule? The numbers don’t support that reading. Supervised MK-677 tends to run about $50 to $150 a month, which lines up with, rather than exceeds, what unsupervised sellers charge for the identical compound [P5]. What that price is actually buying is the clinical evaluation and pharmacy dispensing the criteria are structured around, so it reads more like getting oversight thrown in than paying extra for it.
Does a research-use-only label protect a tested athlete? No, and this one’s not close. MK-677 sits on both the WADA Prohibited List and the DoD’s Prohibited Dietary Supplement Ingredients List, and no disclaimer sticker changes a substance’s status under an anti-doping code [P5][P6]. A competitor relying on the label to stay clean is relying on nothing.
Does the documented rise in growth hormone mean the drug delivers what it’s marketed for? Not on the evidence so far. Growth hormone and IGF-1 rise consistently, that part is solid, but in a two-year trial the resulting fat-free mass gain produced no improvement in strength or function, and in a one-year trial of 563 patients a roughly 73% IGF-1 rise produced no clinical benefit at all [P1][P3]. The hormone axis is doing something real. What it’s doing for the person taking it is a separate, so far unanswered, question, and that’s exactly the distinction criterion 5 asks a seller to be honest about.
What does MK-677 actually do in the body?
It mimics ghrelin, binds the ghrelin receptor in the brain, and prompts the pituitary to release more growth hormone, which in turn raises circulating IGF-1. People commonly report better sleep and increased appetite, and some report body composition changes over time. The clinical data behind the hormonal mechanism is solid; the data on long-term effects in otherwise healthy adults is much thinner, mostly short trials, so treat “long-term” claims with some suspicion.
Is MK-677 a steroid or a peptide?
Neither. It’s a small synthetic molecule, a ghrelin receptor agonist, also called a growth hormone secretagogue. It doesn’t share a structure with anabolic steroids, and unlike an actual peptide such as sermorelin, it isn’t a chain of amino acids that would get digested if swallowed. That structural quirk is why it comes as a capsule or liquid instead of an injectable.
Does MK-677 increase testosterone?
Not through any mechanism it’s known to work by. It acts on the growth hormone and IGF-1 axis, which is a separate system from the one that regulates testosterone. Some users report feeling better overall and credit hormones broadly, but the available clinical data doesn’t show a reliable testosterone bump from MK-677 on its own. If testosterone is the actual goal, this isn’t the compound for it.
How should MK-677 be taken, and does timing matter?
Trial protocols mostly used a single daily oral dose, often at night, since growth hormone naturally pulses during sleep and the appetite increase is easier to sit through while unconscious. Studied doses ran roughly 10 mg to 25 mg daily. None of that constitutes an approved protocol, though, and anyone considering it should be working with a physician rather than a forum thread. Compounding pharmacies operating under physician supervision, the kind FormBlends is built around, are the accountable way to approach a drug with this kind of safety profile.
References
- Nass R, et al. Effects of an oral ghrelin mimetic on body composition and clinical outcomes in healthy older adults: a randomized trial. Annals of Internal Medicine, 2008;149(9):601-611. Fat-free mass increased about 1.1 kg versus a slight loss on placebo with no improvement in strength or function; insulin sensitivity decreased and fasting glucose rose; increased appetite and transient lower-extremity edema were the most common effects. https://pubmed.ncbi.nlm.nih.gov/18981485/
- Murphy MG, et al. MK-677, an orally active growth hormone secretagogue, reverses diet-induced catabolism. Journal of Clinical Endocrinology and Metabolism, 1998;83(2):320-325. In eight healthy young volunteers on caloric restriction, MK-677 shifted mean daily nitrogen balance to positive (+0.31 g/day) versus negative on placebo (-1.48 g/day). https://pubmed.ncbi.nlm.nih.gov/9467534/
- Sevigny JJ, et al. Growth hormone secretagogue MK-677: no clinical effect on AD progression in a randomized trial of 563 patients (25 mg daily, 12 months), despite a 60.1% IGF-1 rise at 6 weeks and 72.9% at 12 months. Neurology, 2008;71(21):1702-1708.
- Adunsky A, et al. MK-0677 (ibutamoren mesylate) for patients recovering from hip fracture: a multicenter, randomized, placebo-controlled phase IIb study. IGF-1 rose but most functional measures did not improve; the trial was terminated early due to a congestive heart failure safety signal in a limited number of patients, and the authors concluded MK-0677 has an unfavorable safety profile in this population. Archives of Gerontology and Geriatrics, 2011;53(2):183-189.
- U.S. Department of Defense, Operation Supplement Safety: MK-677 (ibutamoren) is an unapproved drug and growth hormone secretagogue, not a SARM but often combined with or mislabeled as one; reported to increase fasting blood glucose and hyperglycemia risk and to affect insulin sensitivity; the FDA cites potential for congestive heart failure in certain patients; on the DoD Prohibited Dietary Supplement Ingredients List and the WADA Prohibited List.
- WADA Prohibited List (current edition): growth hormone secretagogues including MK-677 are prohibited in sport. World Anti-Doping Agency.



